Main Content
Research group Lohoff
Project IRF4 and B cell progeny relationship
The processes leading from disturbed B-cell development to adult B-cell progenitor acute lymphoblastic leukemia (BCP-ALL) remain poorly understood. We recently described Irf4−/− mice as prone to developing BCP-ALL with age. Irf4−/− preB-I cells exhibited impaired differentiation but enhanced proliferation in response to IL-7, along with reduced retention in the IL-7 providing bone marrow niche due to decreased CXCL12 responsiveness. Thus selected, preB-I cells acquired Jak3 mutations, probably following irregular AID activity, resulting in malignant transformation. We demonstrate heightened IL-7 sensitivity due to Jak3 mutants, devise a model to explain it, and describe structural and functional similarities to Jak2 mutations often occurring in human Ph-like ALL. Finally, targeting JAK signaling with Ruxolitinib in vivo prolonged survival of mice bearing established Irf4−/− leukemia. Intriguingly, organ infiltration including leukemic meningeosis was selectively reduced without affecting blood blast counts. In this work, we present spontaneous leukemogenesis following IRF4 deficiency with potential implications for high-risk BCP-ALL in adult humans.
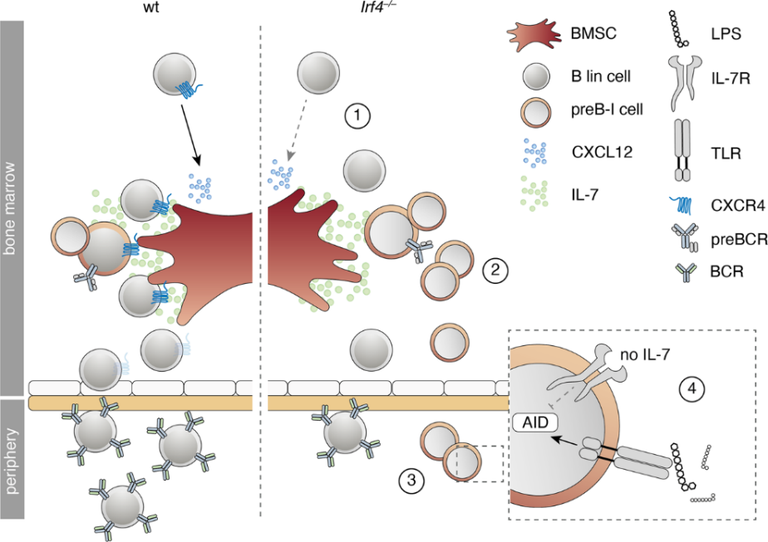
Cartoon summarizing the findings for IRF4 deficient compared to wt B lymphopoiesis. B lineage (lin) cells are less responsive to BMSC-derived CXCL12 due to reduced surface CXCR4 expression (1). Irf4−/− preB-I cells exhibit impaired differentiation and IL-7 dependent hyperproliferation (2). Irf4−/− preB cells escape into the periphery (3), where a combination of IL-7 deprivation and danger-associated molecular patterns (such as LPS) might induce AID expression (4), fueling mutagenesis.
IRF4; MASS CYTOMETRY
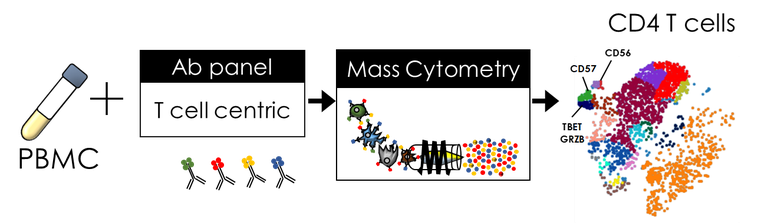
Transcription factor IRF4 plays an important role in different immune-mediated diseases including IBD, asthma, and EAE. Interestingly, primary deficiency of IRF4 avoids canonical T-cell subset differentiation, namely Th2, Th9, and Th17, and mice with such deficiency are resistant to these diseases. Nevertheless, the role of IRF4 after establishment of subsets and disease progression is still unknown, leading to a limitation of appropriate and successful treatment. IRF4 requirements could be analysed by CD4+ specific delayed IRF-deletion once clinical manifestations and cell subsets are settled during IBD or asthma. Among the relevant techniques that could help to answer these questions are FACS, NGS, and CyTOF®, being the latter of huge advantage in the identification of specific CD4+T cell sub-phenotypes. Patients with specific cell subset identification could benefit from a more personalized therapy avoiding the undesirable side effects. CD56 is a marker normally used to identify NK cells (in combination with CD16). When found on other lymphocytes, namely CD3+ T cells, that CD56 expression is associated with enhanced cytotoxicity and proinflammatory function. A deep phenotypic profiling of CD56+ T cells and their subsets has not been fully described. Therefore, we aimed on describing in detail the phenotypical characteristics of these cells also in air dust allergy.
c
Cartoon summarizing the workflow for phenotypical characterization of CD4 T cell subtypes.
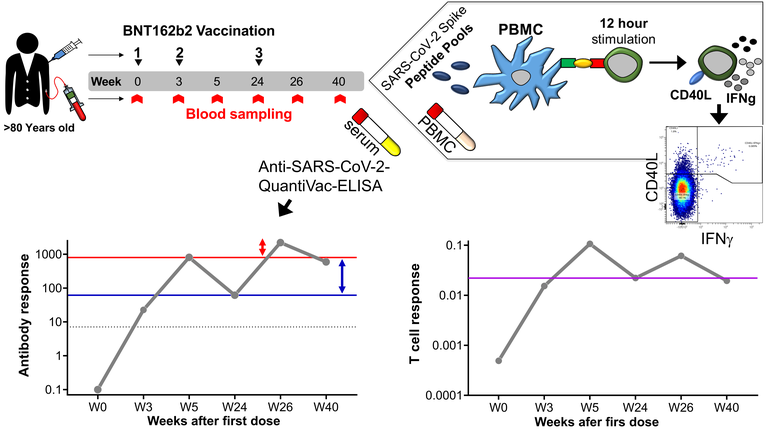
COVID-19
A third mRNA-based booster vaccination is the currently favoured strategy to maintain protection against SARS-CoV-2 infection. Yet, significant waning of specific immunity within 6 months after two doses, along with a higher incidence of breakthrough infections associated with the time elapsed since the second dose, raise concerns regarding the durability of immunity also after the booster vaccination. Based on our observations, a third dose of BNT162b2 in older adults induces a durably escalated humoral response in the bulk of vaccinees for at least three months, indicating longer lasting humoral immunity. Peak virus-specific T-cell frequencies were not further increased by a 3rd dose, and average per-cell production of IFNγ remained not only unaltered but also remarkably lower than in recovered donors of similar age. Thus, even a 3rd BNT162b2 dose failed to induce durably enhanced quantities of spike-specific T cells and a functional quality reached after natural infection. At least in older adults, the durability and quality of vaccine-induced immunity should be considered in the recommendation of booster vaccinations, in addition to the severity of breakthrough SARS-CoV-2 infections caused by current and future viral mutants.